Most important takeaways…
- Respiratory therapists earn roughly $36,000 more per year than medical assistants.
- MA training takes under a year; RT programs require about two years.
- Both fields are projected to grow faster than average through 2034.
Compare education requirements, salaries, daily duties, and career growth to decide which healthcare role fits you best.
Healthcare hiring continues to accelerate across the U.S., yet these two career paths land in very different places. Medical assistants earn a median of $44,200 per year and can start working after less than a year of training. Respiratory therapists earn roughly $80,450, but the entry point is an associate degree that typically takes two years, plus mandatory state licensure.
MAs are outpatient generalists, splitting time between clinical tasks and front-desk administration. RTs are specialized clinicians who manage ventilators, treat COPD exacerbations, and respond to codes in hospital ICUs. The gap in pay, training length, and daily responsibilities is substantial, and so is the commitment required to bridge it.
Medical assistants are the versatile multitaskers of outpatient care; respiratory therapists are the focused specialists who manage breathing in high-stakes settings.
During a typical MA workday, an MA might schedule appointments, update electronic health records, take vital signs, assist with minor procedures, draw blood, or give injections. This broad skill set makes them indispensable generalists. Their medical assistant training emphasizes flexibility, and many employers value MAs who can seamlessly switch from the front desk to the exam room. That jack-of-all-trades role means no two days look exactly alike, but it also means working closely under the supervision of a physician or nurse.
Respiratory therapists (RTs) provide advanced cardiopulmonary care, mostly in hospitals, intensive care units, and emergency departments. Their work is highly specialized: they manage mechanical ventilators, administer aerosol medications, perform diagnostic tests like pulmonary function studies and arterial blood gas analysis, and respond to codes and rapid response calls. RTs often work with a high degree of autonomy under clinical protocols, making critical decisions about oxygen therapy and airway management. While an MA supports a provider, an RT is frequently the expert directing respiratory care. They must think fast, often making independent clinical judgments that directly affect patient survival and recovery.
According to the Bureau of Labor Statistics, roughly 750,000 medical assistants and 130,000 respiratory therapists are employed across the United States, a size difference that reflects MA's role in nearly every outpatient setting and RT's concentrated hospital presence. Both careers are projected to grow much faster than the average for all occupations, driven by an aging population and increasing demand for healthcare services. Whether you're drawn to the breadth of an MA's day or the depth of an RT's specialty, each path offers strong long-term prospects.
The pay gap between medical assistants and respiratory therapists is significant. Based on 2024 data from the Bureau of Labor Statistics, respiratory therapists earn a median salary roughly $30,000 higher than medical assistants nationally. That difference holds across nearly every state. The table below compares median annual salaries and total employment for both occupations, sorted by the highest-paying states for respiratory therapists. Keep in mind these figures reflect all workers in each occupation, not just new graduates.
| State | RT Median Salary | RT Total Employment | MA Median Salary | MA Total Employment |
|---|---|---|---|---|
| New Jersey | $98,020 | 3,200 | $46,280 | 22,530 |
| Washington | $97,150 | 1,850 | $55,120 | 18,430 |
| Massachusetts | $96,940 | 2,140 | $48,540 | 16,210 |
| Oregon | $96,130 | 1,410 | $49,900 | 11,610 |
| Hawaii | $94,670 | 310 | $48,820 | 3,830 |
| Alaska | $94,210 | 170 | $51,860 | 2,420 |
| Minnesota | $88,040 | 1,190 | $49,380 | 9,930 |
| Delaware | $87,380 | 410 | N/A | N/A |
| Maryland | $85,570 | 1,890 | $45,060 | 14,700 |
| New Hampshire | $83,620 | 390 | $48,040 | 2,990 |
| Rhode Island | $83,600 | 250 | $45,820 | 3,270 |
| Connecticut | $83,250 | 1,540 | $46,500 | 9,750 |
| Wisconsin | $82,160 | 1,940 | $47,610 | 12,900 |
| Georgia | $81,890 | 5,030 | N/A | N/A |
| Illinois | $81,310 | 5,450 | $45,490 | 22,990 |
| Montana | $80,950 | 390 | $45,440 | 2,290 |
| Colorado | $80,690 | 2,070 | $47,270 | 12,910 |
| Florida | $79,710 | 8,840 | N/A | N/A |
| Virginia | $79,600 | 2,960 | N/A | N/A |
| Nevada | $79,510 | 1,420 | $43,450 | 7,440 |
| Maine | $79,330 | 450 | $46,540 | 4,120 |
| Arizona | $79,290 | 3,070 | $45,440 | 23,300 |
| Utah | $78,990 | 1,020 | N/A | N/A |
| Nebraska | $78,880 | 820 | $46,080 | 2,560 |
| Vermont | $78,760 | 230 | $45,330 | 1,090 |
The real texture of a career shows up in the daily work, not just the job description. A medical assistant's day is built around clinic flow and patient throughput, while a respiratory therapist's day is anchored in high-stakes pulmonary care and life-support technology. The two roles share a handful of clinical touchpoints, but the bulk of their responsibilities diverge sharply.1
These tasks fall almost entirely to the administrative medical assistant. Respiratory therapists rarely handle front-office duties.
Both clinical medical assistants and RTs interact directly with patients and carry out basic clinical responsibilities, though the context varies.
These duties fall exclusively to respiratory therapists and require advanced training.
The physical setting and emotional pace could not be more different. Medical assistants typically work in clean, well-lit outpatient clinics, physician offices, or ambulatory surgery centers, although some also find medical assistant jobs in hospitals. The atmosphere is structured, with predictable hours and regular patient turnover. Respiratory therapists, by contrast, spend much of their time in intensive care units, emergency departments, and neonatal ICUs. The work is fast-paced, often critical, and can involve responding to codes while a patient's breathing is supported by machinery. This environment demands rapid decision-making and the ability to stay calm when seconds count.
How long does it take to become a medical assistant versus a respiratory therapist, and what will the training actually cost?
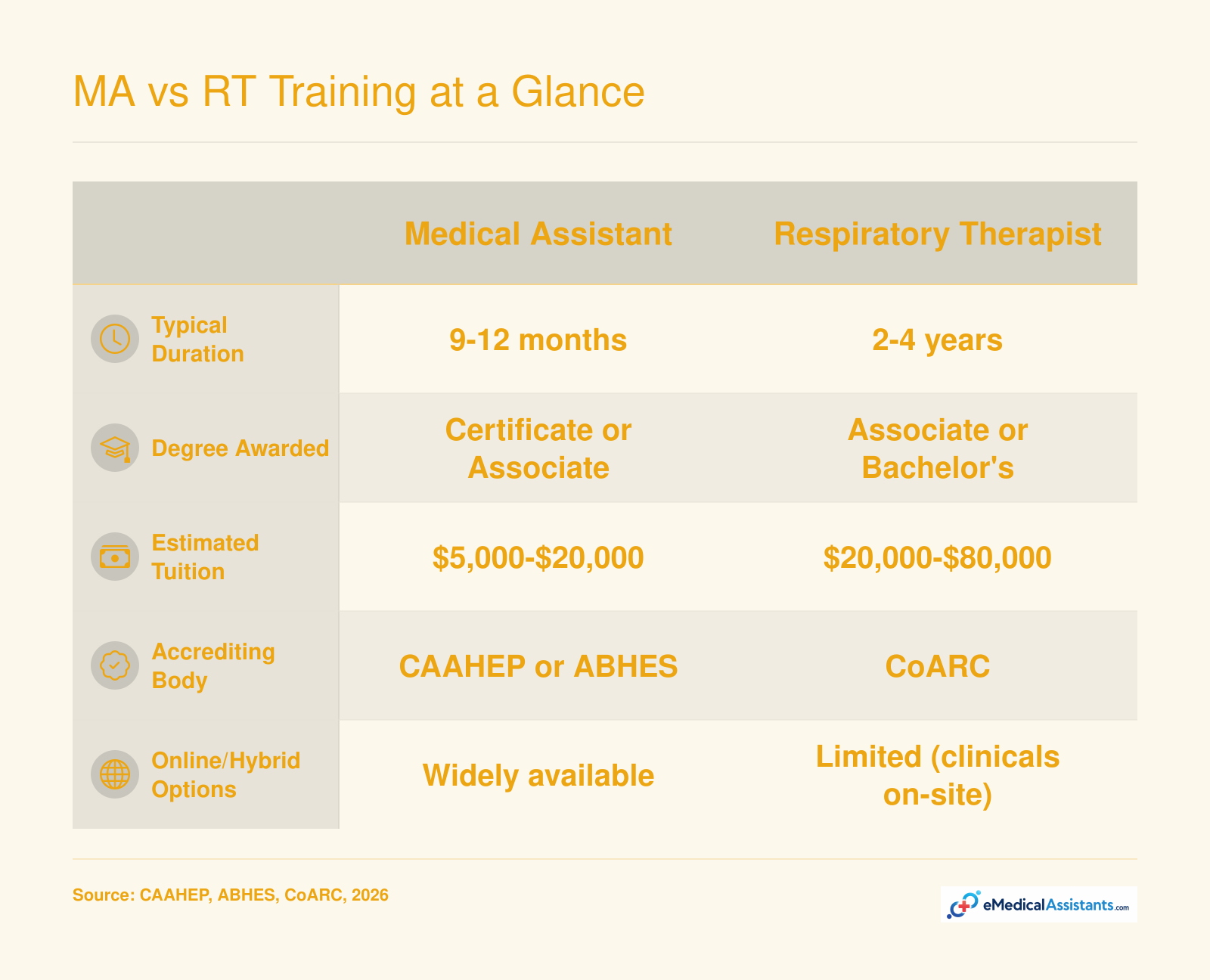
Medical assisting courses (certificate and diploma programs) are designed to get you working fast: most run 9 to 12 months.1 If you choose an associate degree in medical assisting, plan on roughly two years, though that path is less common for entry-level roles. Respiratory therapy programs are a two-year commitment at minimum , the standard credential for licensure is an associate degree, which takes about 24 months of full-time study. For those looking to advance later, bachelor’s degree completion programs in respiratory therapy add another 18 to 24 months but are typically pursued after you’re already working.
Costs vary widely by school type and location, but here’s a realistic look at what you might pay: - Medical assistant certificate/diploma: Community colleges often charge $2,500 to $11,000 total1, while medical assistant trade schools can run $5,000 to $18,000. National extremes dip as low as $1,500 and can reach $20,000. Low-cost online medical assistant programs may come in around $900 to $1,500, though you’ll want to verify hands-on lab components.3 - Medical assistant associate degree: These programs typically cost $8,000 to $32,100 depending on in-state versus out-of-state rates.4 - Respiratory therapist associate degree: In-district community college programs often range from $12,000 to $24,000.1 Private or out-of-state programs can stretch from $25,000 to $40,000.1 - Respiratory therapy bachelor’s degree completion: Already-certified therapists can expect $8,000 to $20,000 for an online or hybrid BSRT program.1
These figures cover tuition, but remember to budget for textbooks, background checks, drug screens, uniforms, and certification exam fees. Financial aid is widely available, and many schools offer payment plans.
For medical assistants, graduating from a CAAHEP- or ABHES-accredited program is what allows you to sit for the CMA (AAMA) exam, though some employers accept other certifications from non-accredited routes.1 Respiratory therapy is non-negotiable: you must complete a CoARC-accredited program to be eligible for the NBRC credentialing exams that lead to state licensure.1 Always check a program’s accreditation status before enrolling.
Both fields require a high school diploma or GED, but the similarities stop there. Medical assistant programs usually have no college-level prerequisites, and a clean background check and up-to-date immunizations are the main gatekeepers.1 Respiratory therapy programs are more selective. You’ll likely need to complete college-level anatomy and physiology, English composition, math (often college algebra), chemistry, and microbiology before you can even apply. Many programs also enforce a minimum GPA of 2.5 to 3.0 in those prerequisite courses.1
That’s a big reason why students often ask: “Is respiratory therapy school harder?” The honest answer is yes, in terms of academic rigor. RT curricula are science-heavy, clinically competitive, and fast-paced, with no room to sidestep subjects like cardiopulmonary physiology or mechanical ventilation. Medical assisting school isn’t without challenge , you’ll learn clinical skills and administrative software in a dense timeline , but the barrier to entry and the depth of science content are noticeably lighter.
Before committing to a program, it helps to see how medical assistant and respiratory therapist training stack up on the factors that matter most: time, cost, credentials, and flexibility. Use this side-by-side snapshot as a quick decision aid.
Voluntary credentials versus mandatory state licensure: that single distinction shapes almost everything about how medical assistants and respiratory therapists enter and advance in their careers. Understanding each profession's requirements will help you plan the right timeline and budget for your goals.
Medical assistants do not need a state license anywhere in the United States. Certification is technically voluntary, but calling it optional can be misleading: most employers strongly prefer, and many outright require, a nationally recognized credential, and it's rarely possible to work as an MA without certification. The three most common options are:
A handful of states add another wrinkle. Some limit the clinical tasks a medical assistant can perform, such as administering injections or drawing blood, unless the MA holds a recognized certification. Even where the law is silent, carrying a credential signals competence to hiring managers and can open the door to higher starting pay.
The respiratory therapist path is considerably more regulated. You must first graduate from a program accredited by the Commission on Accreditation for Respiratory Care (CoARC), then pass the Therapist Multiple-Choice (TMC) exam administered by the National Board for Respiratory Care (NBRC). Passing earns you the Certified Respiratory Therapist (CRT) credential. A higher cut score on the same exam, combined with a Clinical Simulation Exam, qualifies you for the Registered Respiratory Therapist (RRT) designation. Worth noting: the NBRC is transitioning to a single RT credential by 20272, which will simplify the process going forward.
Once credentialed, you must obtain a state license in 49 states plus Washington, D.C.1 Alaska is currently the only state that does not require licensure, though employers there may still expect NBRC credentials.
Several states layer on additional steps beyond passing the NBRC exam:
These state-level differences matter if you plan to relocate or work near a state border. Always check your target state's licensing board before you apply.
The heavier regulatory framework around respiratory therapy is not just bureaucracy for its own sake. Licensed professions generally command higher wages because the barriers to entry are steeper and the scope of practice is more clearly defined. When every practitioner in a field must meet the same education, exam, and licensure standards, it strengthens public trust and professional standing. For medical assistants, the voluntary nature of certification keeps the entry bar lower, which is an advantage if you want to start working quickly, but it also contributes to lower average pay and less standardized career protections.
If you are weighing these two careers, think of credentialing as an investment. A medical assistant credential can be earned in a matter of months and opens clinical doors fast. An RT license takes longer and costs more upfront, but the payoff in salary, job security, and professional recognition is substantial.
Many medical assistants wonder if they can transfer into other professions, such as respiratory therapy, without starting over. The short answer: formal bridge programs that let you shave months or years off an RT degree do not exist for MAs right now.1 However, your MA background is far from wasted. The knowledge you've already built in medical terminology, patient communication, and basic clinical skills gives you a head start in the classroom and at the bedside.
Direct course-for-course credit from a medical assisting certificate or diploma into a respiratory therapy associate degree is rare. Most RT programs require regionally accredited college-level science prerequisites like Anatomy & Physiology I and II, Microbiology, and Chemistry. If you completed those courses at a regionally accredited college and they were taken within the last 10 years, they may transfer.2 Every school sets its own policy, so a transcript evaluation is the essential first step. Some schools, like Tidewater Community College's Bridge to Health Care program, actively support clinical MA program completers who want to enter respiratory therapy. They help with prerequisites and strengthen applications, though it isn't a shortcut to the degree itself.3
The typical path takes 3-4 years for a working medical assistant.2 You'll need a high school diploma or GED, complete all prerequisite coursework, then earn an associate degree from a CoARC-accredited respiratory therapy program. After graduation, you must pass the Therapist Multiple-Choice (TMC) exam and the Clinical Simulation Exam (CSE) to earn the Registered Respiratory Therapist (RRT) credential, which is required for state licensure in most cases.4 Your MA experience often earns you valuable admission points, especially if you can demonstrate strong patient care skills and a history of clinical discipline.2
Quitting your job to return to school full-time isn't always feasible. Many RT programs offer evening, weekend, or part-time tracks designed for working adults. Financial aid, including federal grants and loans, is available for accredited programs, and some healthcare employers provide tuition reimbursement. Talk to your employer's human resources department about any tuition assistance benefits. The combination of academic support and your on-the-job stamina can make the transition both financially and logistically doable.
In the end, moving from medical assistant to respiratory therapist is absolutely achievable. Your clinical foundation doesn't vanish when you enroll in an RT program; it makes you a stronger, more confident applicant who already understands how to put patients at ease.
One career offers a predictable 9-to-5 office rhythm with weekends and holidays off; the other places you in the 24/7 heartbeat of a hospital, where 12-hour shifts and on-call codes are part of the job. What a medical assistant does each day differs dramatically from a respiratory therapist's routine, and those differences shape everything from your energy level at the end of a shift to how you plan your life outside work.
Medical assistants are overwhelmingly found in physician offices, outpatient clinics, and ambulatory care centers. The setting is usually well-lit, climate-controlled, and organized around scheduled appointments. By contrast, respiratory therapists work primarily in hospitals, inside general medical-surgical floors, intensive care units, emergency departments, and neonatal ICUs. Some RTs also provide home health visits for patients on long-term ventilators, but the core of the profession lives in acute care.
Most medical assistants work five eight-hour weekday shifts, roughly 8:00 a.m. to 5:00 p.m., Monday through Friday. Weekend work is rare in office-based roles, and major holidays are generally off, often paid1. The routine is steady and predictable, which is a major draw for people with young children or fixed personal commitments.
Respiratory therapists, on the other hand, face a rotating or fixed schedule of 8- to 12-hour shifts spanning days, evenings, and nights. Working every other weekend is standard, and a holiday rotation means you’ll be on duty for some of the year’s biggest celebrations. On-call time is common, especially for emergency response and code blue teams. Practitioners often say that while the work is deeply rewarding, the irregular hours can make it tough to maintain a consistent sleep schedule or social life.
MAs spend much of the day on their feet, rooming patients, restocking supplies, and assisting with exams, but the physical demands are moderate. The heaviest lifting rarely exceeds 50 pounds, such as helping a patient transfer from a wheelchair2. Infection risk is real but relatively controlled in outpatient environments.
For RTs, physical demands climb significantly. You may need to lift or reposition patients, stand for hours at the bedside in an ICU, and wear full protective gear during aerosol-generating procedures. The risk of exposure to respiratory pathogens is inherently higher, making infection prevention a constant focus.
Seasoned MAs often cite the consistent schedule as a core reason they stay in the field, one of the key pros of being a medical assistant. You can plan a weekend getaway or a weeknight dinner without last-minute schedule changes. RTs, however, describe a more unpredictable rhythm: a 12-hour night shift might transition into a morning of emergency calls, and the emotional intensity of critical care can leave you drained. Yet many RTs also thrive on the variety and feel that the high-stakes environment creates a strong team bond. Ultimately, the choice comes down to whether you prefer a structured, lower-acuity workday or you’re drawn to the adrenaline and unpredictability of hospital-based respiratory care.
Job growth projections give a practical sense of how many new positions a field will add and how easy it may be to find work after training. Both medical assisting and respiratory therapy are expanding faster than the average for all occupations, but the scale and drivers differ sharply.
Medical assistants are in a strong growth category. According to the Bureau of Labor Statistics, employment is projected to increase 12 percent from 2024 to 20341, which is much faster than the average across all jobs. That translates to roughly 101,200 new positions, pushing total employment from about 811,000 to over 912,000. Annual openings, including replacements, are expected to top 112,0001, reflecting high turnover and ongoing demand.
What drives this? An aging population needs more preventive and chronic care, and outpatient settings such as clinics, group practices, and ambulatory surgery centers are expanding rapidly. Medical assistants are the backbone of many of these sites, handling both clinical and administrative tasks, so their growth is tied directly to the shift toward outpatient care.
Respiratory therapists are part of the healthcare practitioners and technical occupations group, which is projected to grow 7.2 percent from 2024 to 2034, faster than the average for all jobs2. While the BLS does not provide a single projection number for respiratory therapists, private estimates suggest the field will add around 20,000 new positions over the decade. The aging population contributes here too, as conditions like COPD, pneumonia, and sleep apnea become more prevalent. Advances in neonatal care and a growing emphasis on pulmonary rehabilitation further support demand.
The absolute numbers tell a clear story: medical assistants are projected to gain over 100,000 new roles, while respiratory therapists may add roughly one-fifth as many. This doesn't mean one career is better; it reflects the size of each profession. Medical assisting, with eight times the workforce, has more churn and broader geographic needs. Respiratory therapy is a smaller, specialized field concentrated in hospitals and skilled nursing facilities.
For job security, both fields offer solid footing. Medical assistants enjoy wider geographic flexibility: you can find work in nearly every community, from rural clinics to large health systems. Respiratory therapists may have fewer total openings but often stronger job security in hospital markets where specialized skills are harder to replace. If you prefer outpatient variety and broader location options, medical assisting offers more roles. If you want to work in critical care and can target metro or suburban hospitals, respiratory therapy offers steady, high-demand opportunities.
Did you know? The Bureau of Labor Statistics projects respiratory therapist jobs will grow 12% from 2024 to 2034, much faster than the average for all occupations, driven largely by an aging population needing care for chronic conditions like COPD and sleep apnea.
The right path hinges on your timeline, your budget, and the type of patient care you find most rewarding.
If you want to get into healthcare fast, minimize training debt, and prefer a steady routine, medical assisting gives you the shortest runway. If you are willing to spend two years in school for a meaningful pay increase and you thrive under pressure while caring for critically ill patients, respiratory therapy is likely the better match.
Medical assisting can also open many doors as a stepping stone, letting you earn a paycheck while deciding if respiratory therapy is your ultimate goal. Just keep in mind that switching to RT means re-enrolling in a full accredited respiratory therapy program; your MA background does not shorten that educational commitment.
To find the right fit, reach out to admissions counselors at accredited MA and RT programs. They can walk you through real job placement numbers, clinical expectations, and which credential is most in demand in your local market.
Below are some of the most common questions people ask when weighing a medical assistant career against respiratory therapy. For the most current numbers, always check official sources rather than secondhand estimates.
Money, time, and setting are what separate these two paths. Respiratory therapists earn roughly 85% more than medical assistants, but that pay bump comes after two years of training instead of one, and it lands you in the higher-pressure environment of a hospital or ICU rather than a calmer outpatient clinic.
Neither path is objectively better. It comes down to what you value: getting to work fast with minimal debt, or investing an extra year for stronger pay and a more clinical, high-acuity role. Be honest about your tolerance for stress and shift work, and ask yourself, 'Am I Cut Out for Medical Assisting?' before you commit.
Ready to move forward? Explore accredited medical assistant and respiratory therapist programs near you to take the next step.